The Reality of Field-Based Care Teams (And Why Most Tools Fail Them)
Published
April 15, 2026
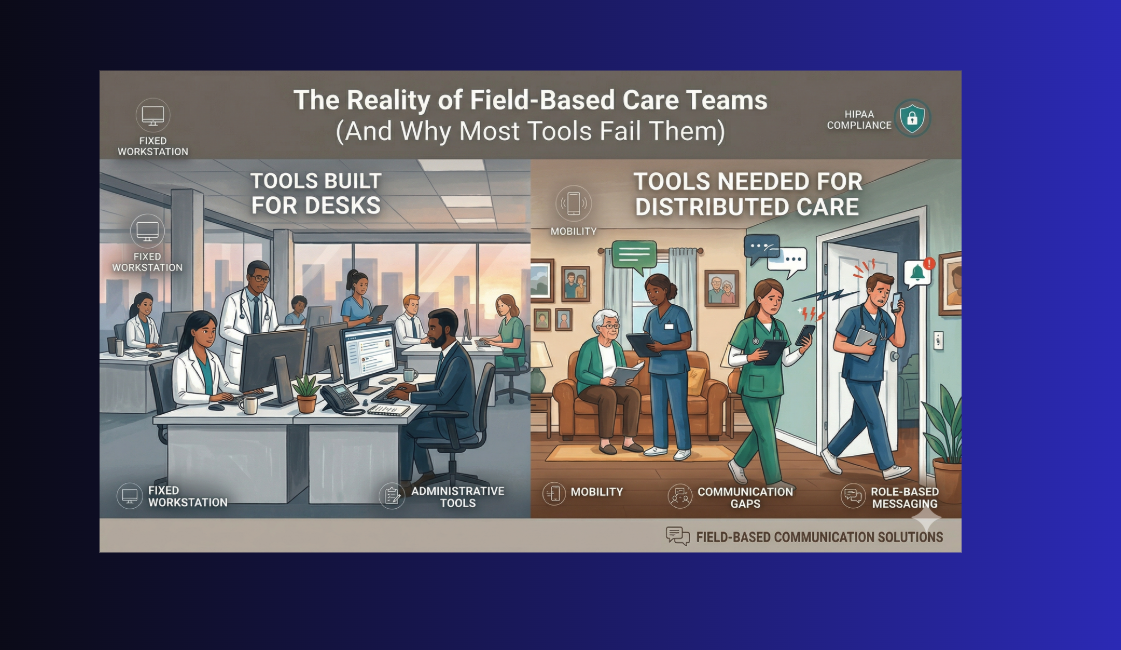
Most communication tools were designed for people who sit at desks, log into the same network, and work in one building. Care-at-home teams do none of those things. And yet most organizations are still trying to run distributed, mobile, high-stakes clinical work on tools built for office workers.
In practice, what tends to emerge is a set of familiar workarounds: shadow communication channels, personal cell phones carrying PHI, and care coordinators spending large portions of their day chasing down information that should have been a single message. These are not isolated edge cases. They reflect a structural mismatch between how most communication tools are designed and how field-based care actually works.
What makes field-based care teams different
Care-at-home organizations operate across a fundamentally different model than hospital or clinic-based care. The care team is distributed across dozens of patient homes at any given moment. No two visits look the same. Clinical situations change between the time a nurse leaves the office and arrives at a patient's door. And the people who need to communicate most urgently are often the least well-equipped to do so.
According to McKnight's Home Care (2023), distributed workforce challenges are among the most persistent operational problems in home-based care settings. Field staff work in isolation from their supervisors and peers, often without reliable access to the back-office systems that hold the information they need. LeadingAge (2023) has highlighted that home-based care operations require communication infrastructure that travels with the clinician, not communication infrastructure that requires the clinician to come to it.
The core characteristics that make field-based care different include:
Constant mobility. Clinicians move between patient homes throughout their shift. They cannot stop and log into a desktop portal to check messages or update care plans.
Real-time decision-making without backup in the room. When a home health nurse identifies a wound that needs a physician order, or a hospice aide encounters a patient in distress, they need answers in minutes, not hours.
High family involvement. Unlike hospital settings, family members are present and actively participating in care decisions. Communication failures become immediately visible to them.
Shift handoffs across geography. When an overnight aide hands off to a morning nurse, the clinical context needs to transfer accurately even though the two clinicians will never be in the same room at the same time.
Regulatory accountability for key touchpoints. Clinical escalations, care plan changes, and substantive family communications need to be documented and defensible, and staff need the tools to make that documentation accurate and timely.
The tools that were not built for this
Most care-at-home organizations are communicating through a combination of tools that were built for entirely different environments. The table below maps what organizations commonly rely on against what field-based care workflows actually require. The gaps are not incidental; they reflect a fundamental design mismatch.
What most teams are using
What field-based care requires
Personal cell phones for urgent clinical messages
HIPAA-compliant mobile messaging with audit trail
Email for care plan updates and shift handoffs
Real-time threaded messaging by patient or care team role
Voicemail for after-hours escalations
Role-based on-call routing that reaches the right clinician instantly
EMR as the primary channel for time-sensitive messages
A real-time communication layer designed to work alongside the EMR, not replace it
Phone calls to update family members one at a time
Automated outbound messaging to families at scale
HIMSS (2024) has documented the growing need for mobile-first care delivery tools, noting that clinicians who spend the majority of their time away from a fixed workstation require communication platforms designed from the ground up for mobile use.
The distinction matters. A tool designed for a desk and later adapted for mobile is a different product than one built from the ground up for someone who is always moving, operating in varied environments, and needs their most common actions to be one or two taps away.
The real cost of the wrong tools
68%
of home health and hospice staff report using personal devices to send work-related clinical messages
HIMSS, 2024
3.2x
higher rate of documentation errors when clinicians use fragmented communication tools
LeadingAge, 2023
52 min
average time per shift field staff spend on communication-related inefficiencies
McKnight's Home Care, 2023
Those numbers translate directly into operational costs. Fifty-two minutes of communication inefficiency per shift, across a team of 40 field clinicians, is over 34 hours of lost clinical time every single day. That is not a workflow annoyance. That is a staffing problem masquerading as a technology one.
Where field-based communication breaks down: a real scenario
Real-world scenario: the handoff that never happened
A home health aide finishes an overnight shift at 7:00 AM. The patient's condition changed during the night: increased pain, reduced mobility, a new concern about skin integrity. The aide documents the visit in the EMR before leaving.
The morning RN arrives at 8:30 AM. She has four other visits scheduled before this one. She reviews the EMR note quickly, but the aide's written documentation does not fully capture the urgency. There is no message. No flag. No follow-up from the overnight care coordinator.
The patient's daughter calls the office at 9:00 AM, upset. She was present overnight and knows the situation has changed. She expected someone to follow up before the next visit. Nobody did.
The problem was not the aide's documentation. It was the absence of a real-time communication layer that could carry the urgency, context, and intent of the handoff in a way that a structured EMR note cannot.
This is the gap that many care-at-home communication tools struggle to close. EMRs and documentation platforms are designed to capture what happened. They are generally not designed to carry the live, contextual communication that field-based care depends on in real time.
What the right tool actually does for field teams
A communication platform purpose-built for care-at-home settings changes the daily reality of field-based work in several concrete ways:
It travels with the clinician
The right tool is mobile-native, not mobile-adapted. It loads fast on a phone, requires minimal taps for the most common actions, and works reliably in the kinds of environments field clinicians actually work in: low-signal rural areas, patient homes with no WiFi, transitions between visits where there are only 90 seconds to send an update.
It routes to roles, not just individuals
Field clinicians should not need to know which specific colleague is on call at 2:00 AM. They should be able to send a message to "on-call RN" or "care coordinator" and have the system route it to the right person automatically. When staff changes happen, the routing adapts. The clinician in the field never needs to update a contact list.
It creates an auditable thread, not a scattered trail
Every message, update, and escalation lives in one place, associated with the patient and the care team. When a supervisor needs to understand what happened during a difficult shift, they do not need to reconstruct a timeline from personal text chains, voicemails, and EMR notes. The communication thread is already there.
It connects the care team to the family
Field-based care does not end at the clinician-to-clinician relationship. Family members are part of the care team in every meaningful sense. A tool that enables proactive, automated outreach to families reduces the inbound call volume that consumes care coordinator time, and it creates a documented record of family communication that protects the organization in the event of a complaint or audit.
How QliqSOFT is built for the reality of field-based care
QliqSOFT designed QliqCHAT specifically for the operating environment that care-at-home teams actually work in. That means mobile-first architecture, role-based messaging that adapts to your on-call schedule, HIPAA-compliant message logging, and a communication layer that sits alongside your EMR rather than trying to replace it.
QliqCHAT Care team messaging
QliqCHAT gives field clinicians a single, HIPAA-compliant channel for every type of clinical communication: peer-to-peer messages, care team threads, role-based escalations, and shift handoffs. It works on any mobile device, routes messages by role and on-call schedule, and creates a complete, auditable communication record for every patient interaction. Field clinicians get faster answers. Supervisors get full visibility. Compliance teams get a documented trail without chasing anyone down.
The shift from fragmented, personal-device communication to a purpose-built platform does not just solve a technology problem. It changes the operational reality for field teams: less time chasing information, fewer missed escalations, cleaner handoffs, and a care team that can focus on the patient in front of them instead of the communication infrastructure underneath them.
See how QliqSOFT works for field-based care teams
Connect with us to learn how QliqCHAT is purpose-built for the distributed, mobile reality of care-at-home organizations.
McKnight's Home Care (2023): Distributed workforce challenges in home-based care operations
LeadingAge (2023): Home-based care operations and mobile communication infrastructure
HIMSS (2024): Mobile-first care delivery trends and clinician communication needs
Frequently Asked Questions (FAQs)
Field-based care teams are constantly mobile, working in isolation across patient homes without reliable access to desktop systems. They need real-time decision support, shift handoffs across geography, and tools that work in low-signal areas - requirements that traditional hospital communication tools weren't designed to handle.
According to McKnight's Home Care (2023), field staff spend an average of 52 minutes per shift on communication-related inefficiencies. Across a team of 40 clinicians, that's over 34 hours of lost clinical time every single day.
EMRs are designed to capture what happened, not to carry live, contextual communication. They lack real-time messaging, role-based routing, and the mobile-first design that field teams need for urgent escalations and shift handoffs.
Essential features include mobile-native design, role-based message routing, HIPAA-compliant messaging with audit trails, real-time threaded conversations, automated family outreach capabilities, and integration with existing EMRs rather than replacing them.
The Author
Krishna Kurapati
Krishna Kurapati is the Founder and CEO of QliqSOFT. He has more than two decades of technology entrepreneurship experience. Kurapati started QliqSOFT with the strong desire to solve clinical collaboration and workflow challenges using artificial intelligence (AI)-powered digital technologies across the U.S. healthcare system.











%20(1).png)
